Secure corridor for infraacetabular screws in acetabular fracture fixation—a 3-D radiomorphometric analysis of 124 pelvic CT datasets
Acetabular fracture surgery is directed toward anatomical reduction and stable fixation to allow for the early functional rehabilitation of an injured hip joint. Recent biomechanical investigations have shown the superiority of using an additional screw in the infraacetabular (IA) region, thereby transfixing the separated columns to strengthen the construct by closing the periacetabular fixation frame. However, the inter-individual existence and variance concerning secure IA screw corridors are poorly understood.
Methods
This computer-aided 3-D radiomorphometric study examined 124 CT Digital Imaging and Communications in Medicine (DICOM) datasets of intact human pelves (248 acetabula) to visualize the spatial IA corridors as the sum of all intraosseous screw positions. DICOM files were pre-processed using the Amira® 4.2 visualization software. Final corridor computation was accomplished using a custom-made software algorithm. The volumetric measurement data of each corridor were calculated for further statistical analyses. Correlations between the volumetric values and the biometric data were investigated. Furthermore, the influence of hip dysplasia on the IA corridor configuration was analyzed.
Results
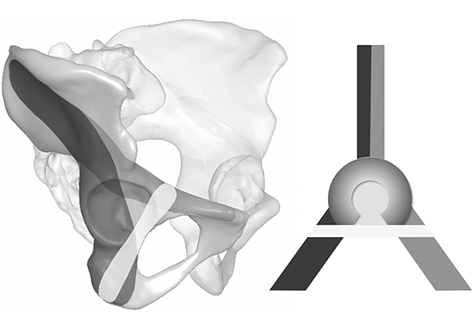
The IA corridors consistently showed a double-cone shape with the isthmus located at the acetabular fovea. In 97% of male and 91% of female acetabula, a corridor for a 3.5-mm screw could be found. The number of IA corridors was significantly lower in females for screw diameters ≥ 4.5 mm. The mean 3.5-mm screw corridor volume was 16 cm3 in males and 9.2 cm3 in female pelves. Corridor volumes were significantly positively correlated with body height and weight and with the diameter of Köhler’s teardrop on standard AP pelvic X-rays. No correlation was observed between hip dysplasia and the IA corridor extent.
Conclusion
IA corridors are consistently smaller in females. However, 3.5-mm small fragment screws may still be used as the standard implant because sex-specific differences are significant only with screw diameters ≥ 4.5 mm. Congenital hip dysplasia does not affect secure IA screw insertion. The described method allows 3-D shape analyses with highly reliable results. The visualization of secure IA corridors may support the spatial awareness of surgeons. Volumetric data allow the reliable assessment of individual IA corridors using standard AP X-ray views, which aids preoperative planning.